High Frequency Oscillatory ventilation (HFOV)
general concept
-
The theory behind HFOV includes the following aspects:
-
Use of supra-physiologic ventilation frequencies and low tidal volumes (less than dead space)
-
Instead of bulk flow (as in conventional mechanical ventilation), gas flow ad therefore ventilation occurs due to
-
Axial dispersion
-
Collateral flow through pores of Kohn
-
Pendelluft phenomenon
-
Taylor dispersion
-
Asymmetric gas profiles,
-
Gas mixing due to pressure-diameter relationship of the bronchi
-
-
Delivery of a constant mean airway pressure (MAP) without the high peak pressures of conventional mechanical ventilation that is directly related to oxygenation
-
Uncoupling of oxygenation and ventilation allowing separate adjustment of either variable
-
-
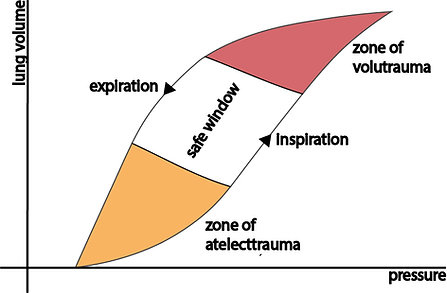
As pressure increases, lung volume increases depending on the tissues' compliance
-
Low pressure go along with atelectasis / collapse, while high pressure cause over distension / volutrauma
-
In order to minimise ventilator-induced lung injury (VILI), HFOV operates in the "safe zone"
-
Note the hysteresis effect between in- and expiration

-
Given the very small tidal volumes during HFOV this mode undulates around a small "safe" window on the expiratory limb of the pressure-volume curve
-
APRV is similar in this as it used high MAPs and small tidal volumes on the inspiratory limb of the pressure-volume curve
Physics involved in gas-exchangE during HFOV


-
As opposed to conventional mechanical ventilation (CMV) which uses bulk flow during in and expiration for gas exchange - HFOV works as a result of a set of physical phenoma
-
The circuit features gas inflow as well as outflow. The mean airway pressure is generated through gradual changes in obstruction to gas outflow via a diaphragm.
-
The membrane generates gas oscillations inside the circuit. The initial amplitude is dampened as it progresses from the membrane down to the alveoli.

General HFOV Ventilator Set-Up
-
The operator sets
-
mPaw (Mean Airway Pressure)
-
Frequency (ƒ)
-
Amplitude (∆P)
-
Inspiratory time (Ti) in % of respiratory cycle
-
-
This results in a waveform that undulates around a mean airway pressure.
-
Half of the amplitude generates positive pressure (inspiration) while the other half generates negative pressure (expiration)

Settings / Variables
-
Increase mPaw
-
Increase FiO2
-
Increase inspiratory time (Ti)
To improve Oxygenation
To improve Ventilation
-
Increase amplitude (∆P)
-
Decrease frequency (ƒ)
-
Decrease inspiratory time (Ti)
-
Deflate ETT cuff
vyaire(TM) 3100A/B

-
This is the most commonly used HFOV ventilator
-
The manufacturing companies have changed over time but the model remains the same
-
There are two models:
-
3100A
-
For children and adults (initially aimed at patients < 35kg)
-
Currently manufactured
-
Consumables available
-
-
3100B
-
For children / Adults > 35kg
-
Currently no longer manufactured
-
Consumables available
-
-